
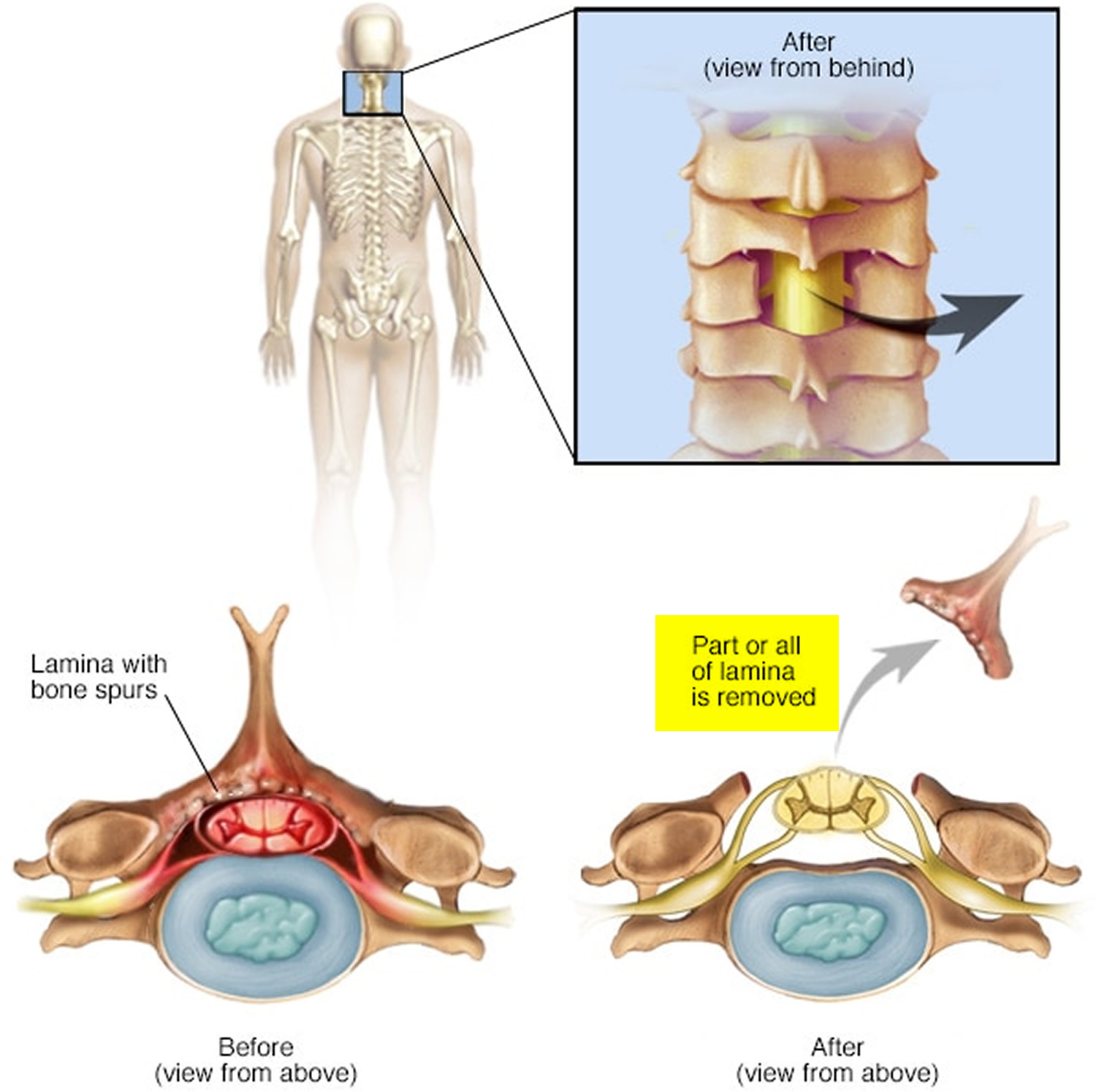
A lumbar laminectomy is a surgical procedure that involves removing a portion of the bone in the spine to relieve pressure on the spinal nerves. Traditionally, this surgery is done through a large incision in the back, which can result in longer recovery times and higher risks of complications. However, advancements in medical technology have allowed for minimally invasive lumbar laminectomies to be performed.
During a minimally invasive lumbar laminectomy, small incisions are made in the back, and specialized tools are used to remove the portion of the bone causing compression on the nerves. This approach results in less muscle and tissue damage, reduced blood loss, shorter hospital stays, and quicker recovery times compared to traditional open surgery.
Minimally invasive lumbar laminectomies are typically recommended for patients with conditions such as spinal stenosis, herniated discs, or degenerative disc disease. While not all patients are candidates for this type of surgery, those who are can benefit from a faster return to normal activities and reduced post-operative pain.
In conclusion, minimally invasive lumbar laminectomy is a safe and effective alternative to traditional open surgery for relieving pressure on the spinal nerves. It offers numerous benefits for patients, including shorter recovery times and lower risks of complications.
Can a laminectomy be done without general anesthesia?
Newer methods are being developed that may allow a laminectomy to be done under local anesthesia as an outpatient. Your healthcare provider will discuss this with you in advance. Generally, a laminectomy follows this process: You will be asked to remove clothing and will be given a gown to wear.

Can laminectomy be minimally invasive?
Minimally invasive bilateral decompressive lumbar laminectomy with a unilateral approach is a less destructive procedure compared to the traditional open bilateral laminectomy.
Who is not a candidate for minimally invasive spine surgery?
Severity of spine condition: Patients with more severe or complex spine conditions may require open surgery instead of MISS. Prior treatments and surgeries: Previous spine surgeries or treatments, as well as the presence of extensive epidural scarring or severe osteoporosis, may limit the feasibility of MISS.
What are the disadvantages of minimally invasive spine surgery?
The risks of minimally invasive spine surgery include: Infection. Excess bleeding. Pain at the graft site.

Is post-laminectomy syndrome a disability?
While not a disability in and of itself, PLS may lead to a lower quality of life, psychological conditions, and disability, especially if it means you can’t work. If you’re unable to work, whether or not you qualify for disability benefits will be decided on a case-by-case basis.
What are the long term problems after a laminectomy?
Arthritis in the facets can cause persistent low back pain even after a successful laminectomy. Osteoporosis. Osteoporosis is a bone condition that causes weak and brittle bones. This condition may cause easy fractures and breakage of bony tissue and may be a risk for laminectomy patients.
Why does my back still hurt after a laminectomy?
Post-laminectomy syndrome causes Persistent pain after a spinal surgery may be due to several causes which include: Nerve root compression. Recurring herniated disc. Joint hypermobility.
Is post-laminectomy syndrome a chronic condition?
Background and objectives. Although not well known, post-laminectomy syndrome (PLS) is an important cause of chronic back pain, which may lead to decreased quality of life, disability and psychological disorders.
Can post-laminectomy syndrome be cured?
Thankfully, post-laminectomy syndrome can often be successfully treated with noninvasive methods such as nerve blocks, spinal cord stimulation, and facet joint injections. Radiofrequency neurotomy is another treatment candidate.


